If you came here just for the video, here you go:
Production (very lengthy) notes below.
This is probably the first prerecorded presentation where I had a hand in the production from blank to finish, and it was not easy for a first. This was not a video recording of a presenter performing a block “live”, which inherently already has its own narration performed naturally to the task. The video recording in this case will naturally follow the flow of the speaker, and ditto with the ultrasound screen recording. Even though you can finish things in one go with this method, there is much more preparation needed beforehand. You need to be ready to record everything as soon as you have a patient; the timing may not be convenient. The recording time is obviously much longer than the actual procedure time and even the final project time. But you potentially have all essential material (with the flow) recorded in just one take.
This was a video where we “shoot first, edit (and narrate) later”. It’s much more convenient, but your video material may not match the the audio (some audio parts may be too long, others too short). This can be mitigated by using freeze frames for the latter and audio breaks for the former. You have complete creative freedom, but “with great power comes great responsibility”. There is a need to think about recording as much as possible, writing (scripting), and post work like in any pure video production. But this was also a medical education video. There is a need to be correct and exact in its details, and therefore the direction and content needs to be thoroughly checked and counterchecked by others superior to me, adding more production time.
To add to the difficulty level, I produced this remotely, with footage recorded by others without me around. I only had a DSL connection for connectivity, but very fortunately my iPhone has an “unlimited” data plan. My workflow was to “continuously” work on the video, produce a version and upload it unlisted to YouTube (as an unlisted file) for the rest of the team to observe and critique. How I uploaded to YouTube was by AirDrop-ping the 500 MB file from the laptop to the phone, then uploading the file to YouTube. Every cycle of exporting, transferring and uploading took around 40 minutes. And for some of the labelling, I was finally forced to use Motion. I may have now graduated from simply using Final Cut Pro. This was my timeline at the end (some of the clips were exported Motion projects, so it’s more complex than it appears):
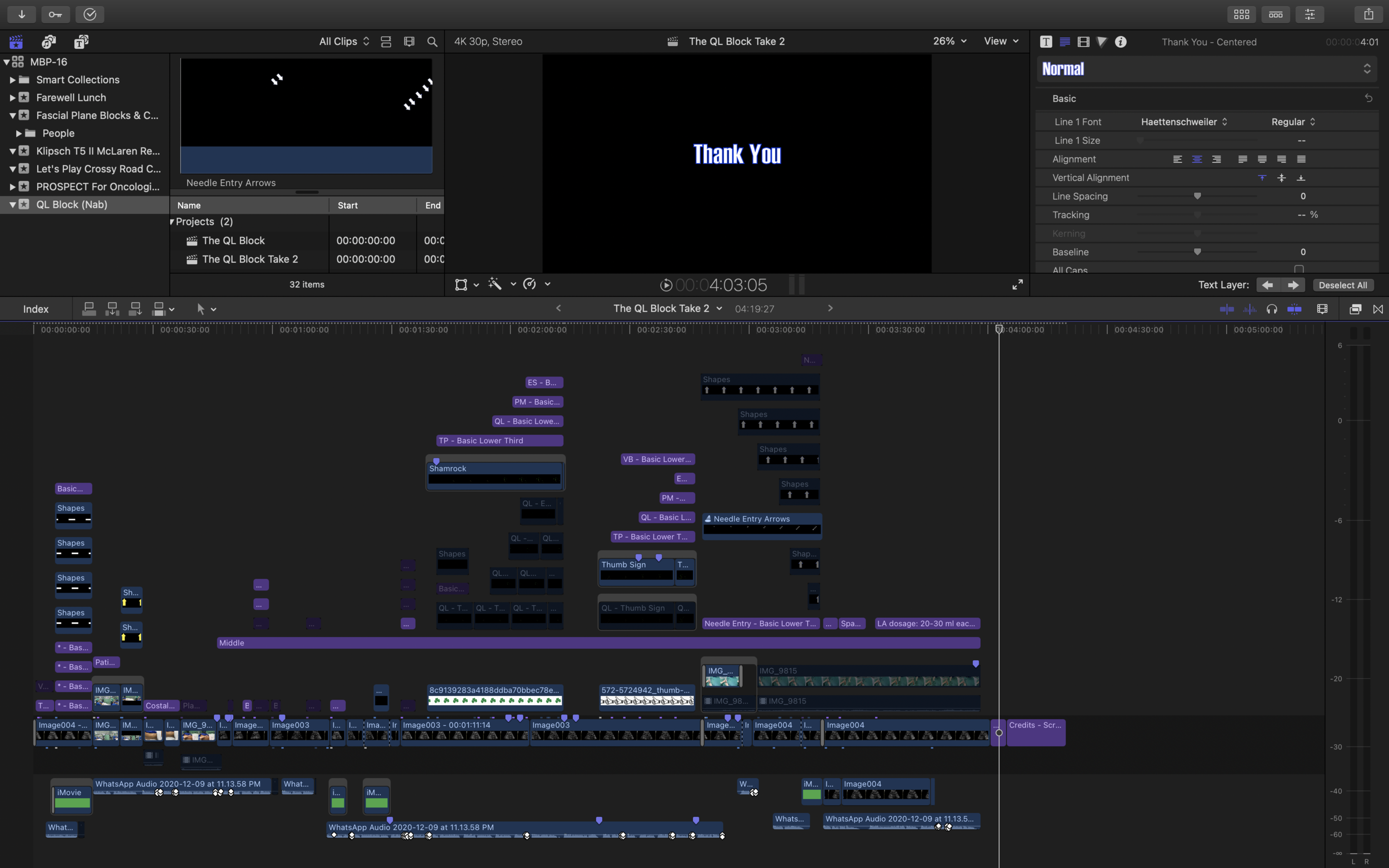
This would not have been possible without my new 16 inch MacBook Pro. Being top spec in terms of it's graphics with the AMD Radeon Pro 5600M (which itself could buy another computer), it allowed me to work without a need to render anything. This saved huge amounts of time and hard disk space; there was no need for additional disk space to save huge render files. Just edit (in H.265 HEVC) and preview it. With my previous 2012 Retina MacBook Pro, this would not have been possible (even with a working screen).
Anyways, back to production.
With a slide presentation converted to video, my job is much easier as someone had done the “what to display” and “what to say” part for me. My job is to “simply” convert this to video with good production values.
With my previous videos the emphasis is always on squeezing out the best audio from the source available to me; bad audio is always worse than bad video. In the case of the recent Emergency Department Regional Anaesthesia webinar, I recorded the audio myself; and in the recently published CME talk, I wasn’t there but my equipment was. With the former I then mixed in portrait videos I recorded myself with the screen recordings to make the final mix; but additional recording was always just a bonus (as simple screen recording would still do). When I started out there was no real video work other that cutting the video into smaller pieces; all I did was audio adjustments, though I must say that censoring people’s faces is not trivial.
This project was more difficult as producing video from scratch means exactly that, from scratch. I had to first imagine how the flow should be, how the narration would be, then get the narration material and make the video (with some video correction, color correction, correct labels and everything else). While being medically correct. And doing my usual clean style of audio production (for this one I slowed the audio by 5%, removed some breath sounds, denoised, cut and matched to the video). By working almost 30 hours for a 4 minute video, difficult is an apt description on working on this. I did make the opening a bit information-dense intentionally. People who want the information can pause the video while those who are not interested can just follow along. One great thing about videos is the ability to watch at your own pace. And the ability to press replay.
I feel that there are measures to speed up the process of making such “video with narration later” medical productions for the future. They have to first be treated just like a feature film. Storyboarding/writing has to be done before recording; this tells you what needs to be recorded; too much footage is never a problem. Going through the script beforehand may highlight needed footage that may be overlooked, along with ensuring that the production brings along the desired message. Labeling of important steps or structures have to be done prior to post to ensure things get done right the first time; this means checking with screenshots and not draft videos. And no matter how trivial, checking things through the clinical supervisor is important and should be done from the beginning and not just often.
As someone who always had content creation aspirations, I’m very excited for doing future works and learning the lessons from them.